
Everything You Need to Know About Medical Cannabis in New York
A primer on medical cannabis in New York State for patients and prescribers; what is medical cannabis; who can prescribe; who can become a patient; the evidence behind medical cannabis

Agapic Answers Member Questions
Every day, Agapic serves others by creating AI assistants that help living beings everywhere reach their health goals. Today, we’re also answering a question asked by an Agapic member, a physician in New York. During a conversation with this member, she asked me about medical cannabis, and I offered to help by researching and answering her questions. Continue reading this post to learn more about medical cannabis. You can also subscribe to Agapic’s posts here. To become a member of Agapic, please join the waitlist here. If you’re already an Agapic member, please reach out to us with any questions you may have related to your own health goals and health journey. We’ll pick some member questions to research and answer, and we hope this helps you and the Agapic community.
A Primer on Medical Cannabis in New York State
1. The current situation in New York
New York legalized the medical use of cannabis on July 5, 2014, and the recreational use of cannabis on March 31, 2021. The Controlled Substances Act of 1970 places cannabis in Schedule I, so, under federal law, it is unlawful for any person to possess cannabis (except in the context of federally approved scientific studies).
2. What is medical cannabis?
Cannabis, including medical cannabis, comprises a single plant species with the scientific name Cannabis sativa L. Cannabis goes by many names, including chronic, hemp, marijuana, pot, and weed.
The term “hemp” is defined in federal and New York law as the plant Cannabis sativa L. with a delta-9 tetrahydrocannabinol (THC) concentration of not more than 0.3% on a dry weight basis. In contrast, the terms “adult-use cannabis” and “medical cannabis” are both used for cannabis that contains more than 0.3% THC.
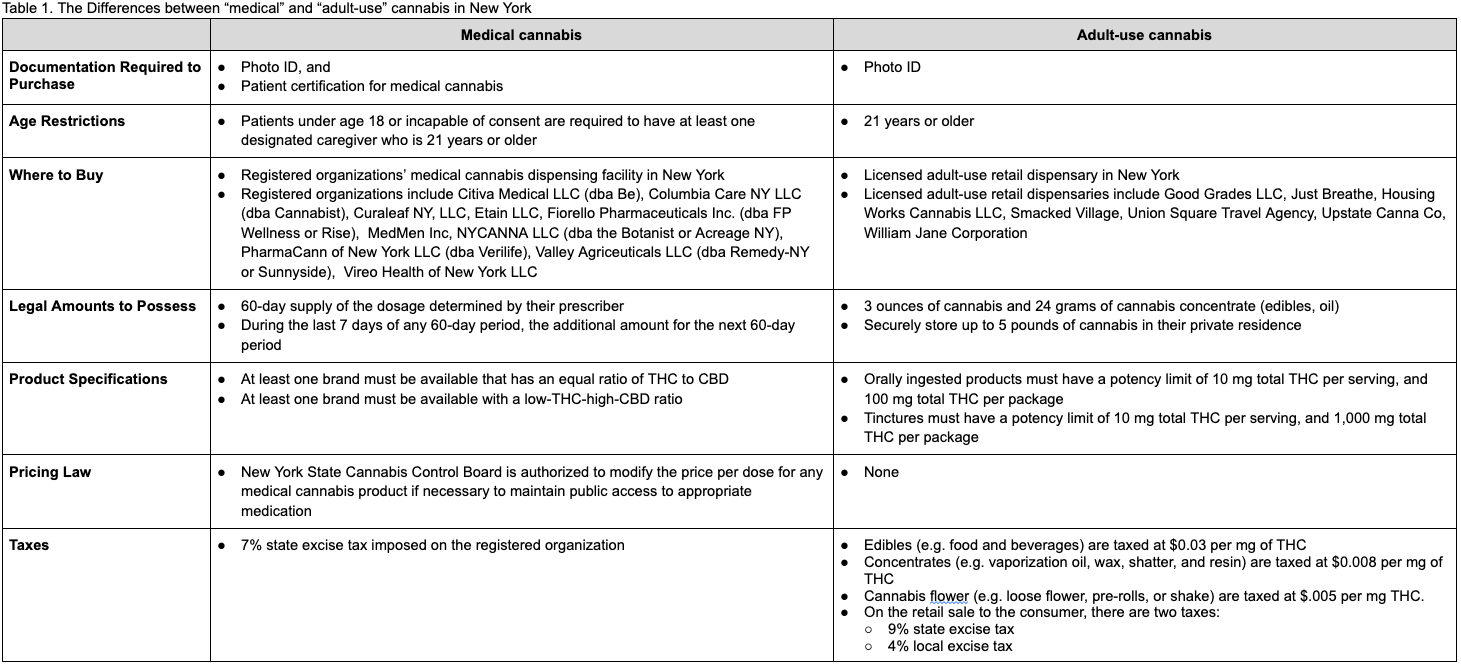
Although “medical cannabis” and “adult-use cannabis” are not different with regards to the plant that’s used, there are differences in terms of how New York law applies, as summarized in the following table:
Who can prescribe medical cannabis?
To issue certifications for patients to receive medical cannabis, health care providers must (1) be licensed, registered, or certified by New York to prescribe controlled substances to humans within the state, and (2) complete at least a two-hour course before they can begin certifying patients for medical cannabis. In practice, courses are 3-5 hours in duration, cost between $145-$229, and several offer CME credits. To certify qualifying patients for medical cannabis, practitioners must use the Medical Cannabis Data Management System (MCDMS) within the Health Commerce System. Medical Cannabis Program certifying practitioners may opt in (or out) to be publicly listed by changing the public list selection in the MCDMS Practitioner Profile section.
Who can become a certified patient for medical cannabis?
To become a certified patient for medical cannabis, you contact your certifying health care provider to see if medical cannabis may help you and is deemed clinically appropriate. Your health care provider will certify you if medical cannabis is appropriate for your condition. Then, with your patient certification and a government issued photo ID, you can purchase medical cannabis at any registered organization’s medical cannabis dispensing facility.
Qualifying conditions include any condition certified by the practitioner. Examples include cancer, HIV/AIDS, amyotrophic lateral sclerosis (ALS), Parkinson’s disease, multiple sclerosis, damage to the nervous tissue of the spinal cord with objective neurological indication of intractable spasticity, epilepsy, inflammatory bowel disease, neuropathies, Huntington’s disease, post-traumatic stress disorder (PTSD), pain that degrades health and functional capability where the use of medical cannabis is an alternative to opioid use, substance use disorder, Alzheimer’s, muscular dystrophy, dystonia, rheumatoid arthritis, and autism.
How is medical cannabis product quality guaranteed? How do they make sure there's no synthetic component, such as K2?
In New York, all adult-use and medical cannabis products must be made in the state. New York requires that all batches of adult-use cannabis and medical cannabis get sampled and tested by authorized firms for a number of specific analytes and contaminants. This includes testing the phytocannabinoid profile (THC, CBD, and more) in cannabis products, and testing for contaminants, including microorganisms, foreign material, metals, microbial impurities, moisture content and water activity, mycotoxins, pesticides, and residual solvents. All cannabis products sold at licensed dispensaries in New York are required to have a label with a link or QR code that brings up the Certificate of Analysis for that cannabis product.
Synthetic cannabinoids, often referred to as K2 and Spice, are illegal in New York and under federal law. Numerous synthetic cannabinoids are specifically listed as Schedule I substances in New York and federal law. In addition, numerous other synthetic cannabinoids meet the legal definition for “cannabimimetic agent,” thus these are also Schedule I substances under both New York and federal law. In New York, adult-use cannabis products and medical cannabis products are explicitly prohibited from including synthetic cannabinoids.
How is the supply of medical cannabis guaranteed?
It is illegal to cross state lines with cannabis, including medical cannabis, therefore New York’s cannabis supply chain is contained entirely within its state borders, which means the supply of adult-use and medical cannabis is also contained within the state.
New York’s medical cannabis supply chain is vertically integrated: the state provides licenses to “registered organizations,” which are then responsible for cultivating, manufacturing and dispensing medical cannabis for certified medical use in New York. New York does allow registered organizations to wholesale manufactured products to one another. Each registered organization can operate up to 8 dispensing sites. In 2015, New York awarded the first five licenses to Columbia Care (NEO: CCHW), Etain, MedMen (OOTC: MMNFF), PharmaCann, and Vireo (CSE: GDNS). In 2017, New York awarded an additional five licenses to Citiva, Curaleaf (CNQ: CURA), Fiorello, NYCANNA, and Valley Agriceuticals. The revenues for four publicly traded registered organizations and information on revenues related to New York state are listed below:
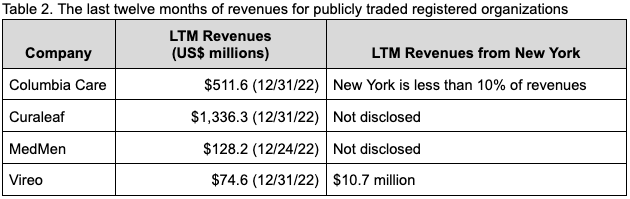
While there is no guarantee for the supply of medical cannabis, there are now a number of large and established registered organizations that are supplying New York’s regulated medical cannabis market.
Is medical cannabis covered by insurance?
Medical cannabis products are not covered by public or private health insurance in New York.
What is medical cannabis used for? What is its effectiveness? What is the evidence behind it? What are the side effects?
Three comprehensive publications on prescribing medical cannabis were examined to answer this question. These publications mention that scientific evidence is limited, studies referenced may have been old or of low quality, advocacy and legalization may be moving ahead of medical due diligence, and that the available research conflicts and has been impeded. Regarding the US, several sources mention that regulatory barriers, including the classification of cannabis as a Schedule I substance, impede the advancement of cannabis research.
In 2021, the UK’s National Institute for Health and Care Excellence (NICE) updated guidelines for cannabis-based medicinal products that include recommendations, summarized below:
Consider nabilone as an add-on treatment for adults (18 years and over) with chemotherapy-induced nausea and vomiting which persists with optimized conventional antiemetics.
Do not offer the following to manage chronic pain in adults: nabilone, dronabinol, THC (delta-9-tetrahydrocannabinol), and a combination of cannabidiol (CBD) with THC.
Offer a 4-week trial of THC:CBD spray to treat moderate to severe spasticity in adults with multiple sclerosis. After the 4-week trial, continue THC:CBD spray if the person has had at least a 20% reduction in spasticity-related symptoms on a 0 to 10 patient-reported numeric rating scale.
Conduct further research on the effectiveness of cannabis-based medicinal products in severe treatment-resistant epilepsy to inform future practice.
In 2018, the European Pain Federation (EFIC) published a position paper on the appropriate use of cannabis-based medicines and medical cannabis for chronic pain management that made several recommendations, summarized below:
Nabiximols oromucosal spray can be considered as part of an add-on individual therapeutic trial for cancer pain without sufficient relief from opioids or other established analgesics.
Cannabis-based medicines can be considered as third-line therapy for chronic neuropathic pain.
In exceptional cases of chronic non-neuropathic noncancer pain, cannabis-based medicines can be considered as an individual therapeutic trial, if all established treatments have failed and after careful analyses and multidisciplinary assessment.
Absolute contraindications include
A history of a hypersensitivity reaction to cannabis-based medicines.
Pregnancy (contemplating or existing) / lactation and children and adolescents, apart from exceptional circumstances.
Relative contraindications include
Current or a history of mental disorder, especially substance abuse and dependence, and psychosis.
Seizures and severe cardiac disorders.
Consider a lower starting dose in elderly patients.
Consider a lower starting dose in patients with renal and hepatic insufficiency.
Do not prescribe cannabis-based medicines to patients taking high doses of opioids or benzodiazepines.
Advise patients not to drive at all if a therapy with cannabis-based medicines is started or modified until a stable dosage for 5–7 days is reached. Advise patients not to drive while under the influence of cannabis-based medicines and not to drink alcohol. Do not prescribe cannabis-based medicines to patients with professional driving (taxi drivers, truck drivers, ambulances).
Recommend a medical assessment for working ability of patients in jobs where there is a potential for harm to oneself or to others (patients operating machines, etc.).
Cannabis based medicines can have both pharmacokinetic and pharmacodynamic interactions with other drugs. Reduce the dosage of other centrally acting drugs as far as possible before cannabis-based medicines are used.
Patients treated with cannabis-based medicines require special attention during the perioperative period.
If a patient is suited for a trial with cannabis-based medicines, start with oral or oromucosal cannabis-based medicines (e.g., dronabinol, nabiximols).
If oral or oromucosal individual cannabis-based medicines (e.g. dronabinol, nabiximols) do not work, a trial of cannabis extract (oil) or inhaled cannabis can be considered.
Advise patients to use medical cannabis as oil extract or via a vaporizer for inhalation (dried cannabis) and not to smoke cannabis. Advise patients to use approved medical devices.
Do not prescribe cannabis flowers with a high (>12.5%) THC content. A dose of no more than one inhalation four times per day to avoid cannabis intoxication and cognitive impairment is recommended.
In 2017, the US National Academies of Sciences, Engineering, and Medicine published a report on the health effects of cannabis that included a number of conclusions, with selected conclusions summarized below:
Therapeutic Effects of Cannabis and Cannabinoids: There is conclusive or substantial evidence that cannabis or cannabinoids are effective:
For the treatment of chronic pain in adults
As antiemetics in the treatment of chemotherapy-induced nausea and vomiting (oral cannabinoids)
For improving patient-reported multiple sclerosis spasticity symptoms (oral cannabinoids)
Respiratory Disease: There is substantial evidence of a statistical association between cannabis smoking and worse respiratory symptoms and more frequent chronic bronchitis episodes (long-term cannabis smoking)
Injury and Death: There is substantial evidence of a statistical association between cannabis use and increased risk of motor vehicle crashes
Prenatal, Perinatal, and Neonatal Exposure: There is substantial evidence of a statistical association between maternal cannabis smoking and lower birth weight of the offspring
Mental Health: There is substantial evidence of a statistical association between cannabis use and the development of schizophrenia or other psychoses, with the highest risk among the most frequent users
Problem Cannabis Use
There is substantial evidence that:
Stimulant treatment of attention deficit hyperactivity disorder (ADHD) during adolescence is not a risk factor for the development of problem cannabis use
Being male and smoking cigarettes are risk factors for the progression of cannabis use to problem cannabis use
Initiating cannabis use at an earlier age is a risk factor for the development of problem cannabis use
There is substantial evidence of a statistical association between:
Increases in cannabis use frequency and the progression to developing problem cannabis use
Being male and the severity of problem cannabis use, but the recurrence of problem cannabis use does not differ between males and females
What are customers saying about the benefits or cons of cannabis?
Looking at WebMD’s and Drugs.com’s user reviews for cannabis, most users find cannabis to be effective for their condition. Looking at the reviews by condition, 28% are for pain, 5% are for weight loss, 3% are for rheumatoid arthritis, 2% are for cancer, and the rest (62%) are “other,” which includes bipolar disorder, muscle spasms, secondary progressive MS, and difficulty sleeping. Users comment that cannabis helps relieve pain effectively. Users have concerns about the legality of using cannabis in their jurisdiction and the cost of cannabis. Some patients report side effects, such as anxiety, heart palpitations, impaired balance, intestinal discomfort, loss of short term memory, panic, and sleepiness.
An example of a positive review, taken from WebMD, follows: “this saved my husbands life...24 years ago my husband was given 3-6 months to live due to lung cancer,I threw away all his drugs that made him a zombie and started him on this treatment..yes it was still illegal.. but when he could keep down food for the first time in months and the pain was much less, he was hungry for the first time in months, he started to put on weight and felt good...Yes I did end up loosing him to the lung cancer..BUT not for 24 years after he was diagnosed ...so why is this not legal?????”
Here is an example of a negative review, also taken from WebMD: “I have Fibromyalgia,PTSD and anxiety. I used a candy and ate half,then at bedtime I put 2 drops under my tongue. I got a HORRIBLE reaction!! I had anxiety,panic,dizzy,heart palpitations,severe heartburn and my chest felt like it was on fire!!! NO MORE for me!!!”
How do you enter medical cannabis prescriptions on I-STOP?
Practitioners and registered organizations are required to use the prescription monitoring program (PMP). Specifically, every practitioner is required to consult the PMP registry prior to making or issuing a certification, and all dispensing sites must consult the PMP registry prior to dispensing medical cannabis to a certified patient. Further, dispensing facilities submit dispensing data to I-STOP within 24 hours. This includes zero reports that identify that there was no product dispensed. Medical cannabis dispensaries in New York have pharmacists on-site to help patients find the right product for their conditions, check for interactions with other medications, and show patients how to use each form of cannabis.
How have crime rates changed in New York since cannabis was legalized?
Reports reviewed to better understand the impact of legalized cannabis on crime mention that the data available for before-and-after comparisons are limited, so conclusions about the effects of legalizing cannabis remain tentative.
In 2021, the Cato Institute updated a study on the effect of state cannabis legalizations, which concluded that, at most, cannabis legalization causes small changes in various outcomes, and that violent crime has not changed significantly. The Cato Institute study indicated that the only area where cannabis legalization has a significant impact is through increasing state tax revenue.
In 2019, a US Department of Justice research project on the impact of cannabis legalization and decriminalization on state justice system resources concluded
Legalizing adult-use cannabis resulted in fewer cannabis related arrests and court cases;
Legalizing cannabis did not have a noticeable impact on indicators in states that bordered those that legalized; and
There were no noticeable indications of an increase in arrests related to transportation or trafficking offenses in states along the northern or southern borders.
What are the New York DMV rules around cannabis intoxication? What percentage in the bloodstream constitutes being intoxicated?
In New York, driving while ability impaired by cannabis, or by the combined influence of cannabis with alcohol or any other drug, is a crime. Even as a certified patient for medical cannabis, if you are impaired while driving, you are at risk of getting a DUI. Additionally, under the open container law, cannabis cannot be consumed or burned by anyone in a vehicle. Further, drivers must store cannabis securely in a trunk or locked glove compartment, and out of reach of individuals under 21. Under federal law, you cannot possess or use cannabis while crossing state or international borders, or on federal lands or property.
In New York, there is no blood alcohol content (BAC) equivalent for cannabis. The state notes that levels of cannabis in the blood rapidly spike after use, and quickly dissipate below detectable levels, with impairment lasting longer than cannabis lasts in the blood. Accordingly, New York has provided select law enforcement officers with specialized training to draw blood while cannabis is still detectable, and to perform other tests to recognize impairment. Regardless of the level of cannabis in the blood, law enforcement officers may base DUI arrests on observed impairment.
About Agapic
Agapic creates AI assistants that help people reach their health goals. You can subscribe to our posts, and join our waitlist to become an Agapic member. If you’re already an Agapic member, please reach out to us with any questions you have related to your own health goals. We will pick some member questions to research and answer, and we hope this helps you and others.
Agapic News Disclaimer
Agapic News provides general information and discussions about health and related subjects. The information and other content provided in this post, website or in any linked materials are not intended and should not be considered, or used as a substitute for, medical advice, diagnosis or treatment. Agapic News does not constitute the practice of any medical, nursing or other professional health care advice, diagnosis or treatment. We cannot diagnose conditions, provide second opinions or make specific treatment recommendations through this website.
If you or any other person has a medical concern, you should consult with your health care provider or seek other professional medical treatment immediately. Never disregard professional medical advice or delay in seeking it because of something that you have read on this website or in any linked materials. If you are experiencing a medical emergency, please call 911 or call for emergency medical help on the nearest telephone immediately.
No physician-patient relationship is created by this website or its use. Neither Agapic nor its employees, nor any contributor to this website, makes any representations, express or implied, with respect to the information provided herein or to its use.
References
CATO Institute. The Effect of State Marijuana Legalizations: 2021 Update. 2 February 2021.
Columbia Care. Form 10-K For the fiscal year ended December 31, 2022. 29 March 2023.
Curaleaf. Consolidated financial statements for the years ended December 31, 2021 and 2020. 7 March 2022.
Curaleaf. Curaleaf Reports Fourth Quarter and Fiscal Year End 2022 Results. 1 May 2023.
Drugs.com. User Reviews for Cannabis. Last accessed 2 May 2023.
European Pain Federation (EFIC). Position paper on appropriate use of cannabis-based medicines and medical cannabis for chronic pain management. 3 August 2018.
Goodness Growth Holdings (Vireo). Form 10-K for the fiscal year ended December 31, 2022. 31 March 2023.
MedMen. Form 10-K for the fiscal year ended June 25, 2022. 9 September 2022.
MedMen. Form 10-Q for the quarterly period ended December 24, 2022. 2 February 2023.
National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids. 12 January 2017.
National Institute for Health and Care Excellence (NICE). Cannabis-based medicinal products. Last updated 22 March 2021.
New York Cannabis Control Board. Repeal of 55-2.2(a)(5) and 55-2.15 of Title 10 NYCRR and addition of Part 130 Cannabis Laboratories to Title 9 NYCRR. March 2023.
New York Cannabis Control Board. Repeal of Part 1004 of Title 10 NYCRR and Addition of Part 113 Medical Cannabis to Title 9 NYCRR. July 2022.
New York Department of Health. Public List of Consenting Medical Cannabis Program Practitioners. Accessed 29 April 2023.
New York Office of Cannabis Management, New York Governor’s Traffic Safety Committee. Cannabis and Driving. 21 March 2022.
New York Office of Cannabis Management. How to Read a Lab Certificate of Analysis for Your Cannabis Product in New York. April 2023.
New York Office of Cannabis Management. Inaugural Annual Report. 2022.
New York Office of Cannabis Management. Marihuana Regulation and Taxation Act. Signed into law 31 March 2021.
New York Office of Cannabis Management. Part 113 – Medical Cannabis APC. September 2022.
New York Office of Cannabis Management. Practitioners. Accessed 28 April 2023.
New York Office of Cannabis Management. Registered Organizations. Accessed on April 25, 2023.
New York Office of Cannabis Management. Required Testing of Each Lot of Adult Use Cannabis and Medical Cannabis Product. 4 January 2023.
New York Office of Cannabis Management. What is in the Law Medical Cannabis. October 2022.
New York Senate. Article 33 Controlled Substances. 30 December 2022.
New York Senate. Senate Bill S7923, Relates to the medical use of marihuana. Signed into law 5 July 2014.
United States Congress, 91st. The Controlled Substances Act: 21 U.S. Code Chapter 13 - Drug Abuse Prevention and Control. Signed into law 27 October 1970.
United States Congress, 115th. Agriculture Improvement Act of 2018. 20 December 2018.
United States Department of Justice. Measuring the Criminal Justice System Impacts of Marijuana Legalization and Decriminalization Using State Data. July 2019.
WebMD. User Reviews For Cannabis. Last accessed 2 May 2023.
Wow. Very thorough and well-researched. Great job!